The shoulder joint complex is made up of four different joints, these are the:
Glenohumeral (shoulder) joint
Acromio-clavicular (AC) joint
Sterno-clavicular (SC) joint
Scapulo-thoracic joint
The glenohumeral (shoulder) joint is the most mobile joint in your body. It is a ball and socket joint made up of the humerus and the scapula. The AC joint connects your scapula to your clavicle (collar bone). The SC joint connects your clavicle to your sternum (breastbone), and is the joint that directly connects your upper limb to your body. The scapulo-thoracic joint is the joint between your scapula and your rib-cage. Although this is not a true joint, the motion between your scapula and rib-cage is very important in maintaining normal shoulder function.
Due to the mobility in the shoulder complex, this region is vulnerable to injury and relies heavily on muscular support to maintain posture and pain free motion. Many different injuries can occur in the shoulder region - the most common ones are outlined in more detail below.


The rotator cuff is the collective name for 4 muscles and their tendons that support the ball of the shoulder joint in the socket of the shoulder blade. The four muscles are:
Supraspinatus
Infraspinatus
Teres Minor
Subscapularis
The shoulder joint (or glenohumeral joint) is a mobile joint that has a very shallow socket. It has been described as the equivalent of a golf ball on a tee. The function of the rotator cuff is to act as dynamic stabilisers to prevent excessive shoulder joint movement. They also help maintain optimum position of the shoulder to allow the strong power driving muscles to function.
Rotator cuff injuries can occur as a result of repetitive overhead activities such as painting, building or lifting. Some occupations are susceptible to this type of injury such as builders, cleaners and general labourers. This leads to degenerative change within the rotator cuff tendons known as tendinopathy. Sometimes, rotator cuff tears may also occur as a result of a single injury such as a fall onto a shoulder, or grabbing onto something to prevent a fall. This type of injury can lead to either a partial or complete rotator cuff tear. Extensive rotator cuff tears may require surgical repair. The risk of rotator cuff injury also increases with age.
Good function of the shoulder also depends on the coordinated movement of the arm in conjunction with the shoulder blade. Subtle changes in this movement pattern can contribute to overloading of the rotator cuff and injury.
Many people recover from rotator cuff disease with physical therapy exercises that improve flexibility and strength of the muscles surrounding the shoulder joint. At Roslyn Physio we regard shoulder problems as an interesting challenge and believe we are very good at resolving shoulder pain. We will first help you by diagnosing the problem, and will then provide a prognosis so you have clear time frame for probable recovery.
We will then treat utilising hands on physiotherapy, including joint mobilisation and exercise therapy to resolve any stiffness, weakness or movement pattern problems that may be causing your pain. Should you require further investigations such as an x-ray or an ultrasound scan to ascertain the severity of your injury, we are able to refer you for these.
Open this file to see commonly prescribed exercises for rotator cuff injuries. These exercises are not designed to replace an assessment and treatment plan from your physiotherapist, and should any of these exercises increase your pain you should stop these immediately and seek help from a physiotherapist.
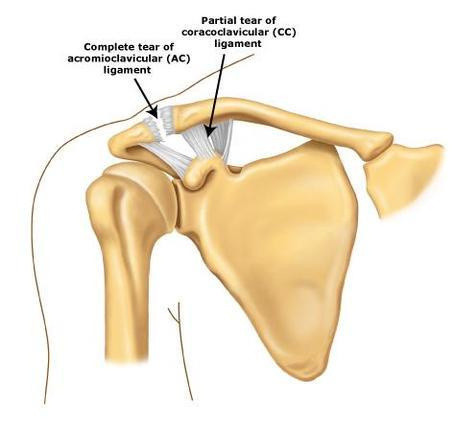
The Acromio-clavicular(AC) joint is formed by the acromion of the scapula (shoulder blade) and the clavicle (collar bone). There are several ligaments which can be of importance in AC joint injuries:
the acromio-clavicualr ligament - or the AC joint capsule.
the coracoclavicular or CC ligament which joins the clavicle to the coracoid process which is another forward protruding part of the scapula. There are two distinct bands to this ligament.
the coracoacromial ligament attaches the acromion process to the coracoid process.
AC joint sprains occur whent the ligaments described above are either partially or completely torn. There are many different grades of AC joint injury ranging from very mild (grade 1) to severe (grade 6) .
The most common way of injuring the AC joint is by landing on the shoulder, elbow, or onto an outstretched hand. When you fall you automatically place your hand out to break the fall. The forces are then transmitted up the wrist and arm to the shoulder joint.
Symptoms of an AC joint injury include pain over the AC joint, a loss of range of motion in the shoulder - especially across your body and above your head, an inability to lie on the shoulder, and swelling/deformity over the AC joint.
Depending on the grade of injury the treatment will vary. It is best to get advice from a physiotherapist to ensure you receive the correct advice. Your injury will typically take 4-6 weeks to heal and over this time there will be a variety of treatment options:
Strapping
Massage
Use of a sling/immobilisation
Active range of motion exercises to increase flexibility
Strengthening exercises for your shoulder and scapula stabilisers
A graduated return to sport and contact training

Shoulder dislocations may either occur as a result of trauma or from an intrinsic loss of ligament support. A true dislocation involves the humeral head (the ball) coming out of the glenoid of the scapula (the socket), and staying out. If the shoulder moves out briefly but relocates on its own, this is known as a subluxation. The shoulder is the most commonly dislocated joint in the body. Most shoulder dislocations occur in a forwards (anterior) direction.
Patients with a previous shoulder dislocation are more prone to further dislocation. This comes about from the tissues being stretched and not healing properly, therefore the shoulder becomes looser than normal. If you are under the age of 20 and sustain a shoulder dislocation you have a higher risk of recurrent dislocation. This may lead to a condition known as shoulder instability.
The signs and symptoms of a dislocated shoulder include:
intense pain
the inability to move the shoulder
a loss of sensation in the arm
marked weakness in the arm
a history of trauma or previous dislocation
the shoulder does not 'look right'
The shoulder is normally relocated with the use of pain medication and should only be done by a trained health professional otherwise there is a change of damaging the shoulder further. Other structures such as your rotator cuff, or the labrum of the shoulder can be damaged with shoulder dislocation. It is important to get the shoulder x-rayed to rule out bony damage to the shoulder and a sling is normally worn to support the shoulder for the first 7-10 days.
Physiotherapy is an important part of rehabilitation following a shoulder dislocation. It is critical that good muscle strength is regained in the shoulder complex otherwise there is a higher chance of further dislocation. Your physio will prescribe a rehabilitation programme following an assessment of your strength and shoulder motor patterns.
This video demonstrates an easy and effective way of providing some support to an unstable shoulder. The technique incorporates a simple shoulder taping along with further taping support for the overhead athlete. Remember that all taping supplies are available at Roslyn Physio.